Safe Staffing
October 29, 2022 2024-11-14 10:43Safe Staffing
Safe Staffing
AFTER TWO DECADES OF FIGHTING FOR STATEWIDE SAFE MINIMUM STAFFING STANDARDS TO REDUCE NURSE BURNOUT AND TURNOVER, ENCOURAGE MORE RNS TO RETURN TO THE BEDSIDE, AND IMPROVE PATIENT SAFETY IN PENNSYLVANIA, OUR LEGISLATION — THE PATIENT SAFETY ACT — PASSED THE HOUSE!
There’s an acute nurse staffing crisis in hospitals across the commonwealth, and it wasn’t created by the pandemic. It started long before COVID-19 even existed. Hospitals have too often tried to cut costs by overloading nurses and skimping on patient care. We can’t count on the hospitals, who are the cause of the problem, to fix it. We need PA state legislators to act to address the staffing crisis in our hospitals.
A growing bipartisan majority of the Pennsylvania House agrees and has signed on as co-sponsors of legislation called the Patient Safety Act (HB106), which would set minimum safe staffing levels for nurses in hospital units across Pennsylvania. But neither the House bill nor the Senate version (SB 240) has been allowed a hearing or a vote in their respective committees.
PLEASE SIGN THIS PETITION URGING PA STATE LEGISLATORS TO ADDRESS
THE STAFFING CRISIS IN OUR HOSPITALS AND ACT ON THE PATIENT SAFETY ACT!
THE PATIENT SAFETY ACT (PA HOUSE BILL 106 + PA SENATE BILL 240)
In 1999, California passed, and in 2004, implemented, the first and still only comprehensive state legislation to limit the number of patients that hospital nurses are permitted to care for at one time. The law has been enormously beneficial for patients and, despite what administrators would have us believe, has not led to any issues in their booming healthcare industry. Pennsylvania’s Patient Safety Act (PA House Bill 106 and Senate Bill 240) is patterned after California’s law. Each bill seeks to limit the number of patients a nurse can be assigned depending on the level of care a patient requires. The standards in the bills are very specific and based on patient acuity. For instance, the nurse-to-patient safe minimum standard set forth in the bills for the ICU is 1:2 or fewer; the standard for presurgical and admissions units or ambulatory surgical units is 1:4 or fewer.
PLUS: Safe Harbor Provisions. Both Pennsylvania bills include protections for nurses from “adverse action by the healthcare facility where the nurse is working when the nurse makes a good-faith requrest to reject an assignment based on the nurses’s own education, knowledge, competence and experience, and an immediate assessment of the risk for patient safety.”
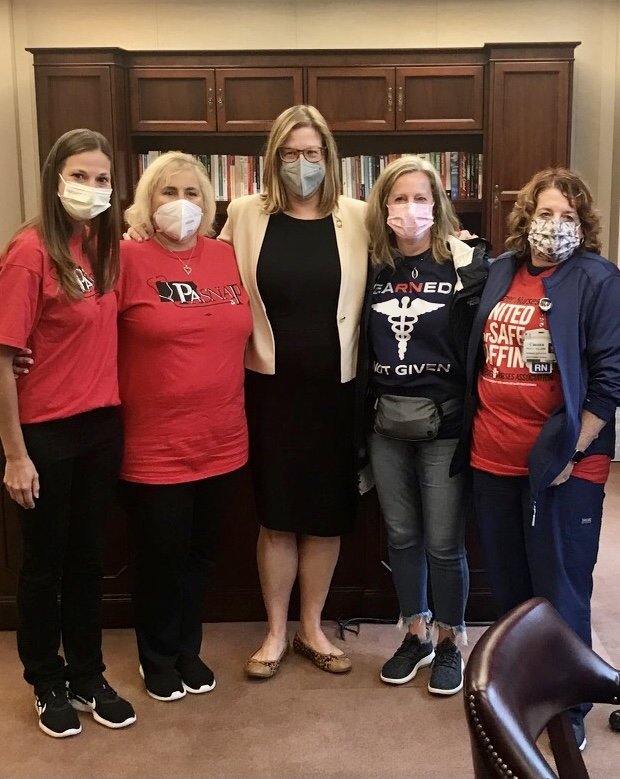
PASNAP members meet with Delco state Rep. Leanne Krueger in Harrisburg.
We stand here today as whistleblowers — not as people looking for an easier day at work but as a group of people with a behind-the-scenes view of what is happening and how the public is put at risk every day.
SHANNAN GIAMBRONE, RN, PASNAP EXECUTIVE BOARDMEMBER
THE RESEARCH
Nurses across the nation have been sounding the alarm for decades: There are simply not enough nurses at the bedside. What this means in ERs and on hospital floors across the commonwealth is that nurses are being asked to care for more patients than is safe for either the patient or the nurse. When nurses are routinely required to care for patients than is safe, it’s called chronic nurse short-staffing, and it’s a crisis for both patients and nurses. Numerous studies over many decades have shown:
"This shortage of nursing care during COVID? It’s the result of hospitals employing too few nurses for decades! And hospital industry representatives will do everything they can to keep it that way."
LINDA AIKEN, PH.D., R.N., THE FOREMOST EXPERT ON NURSE STAFFING IN THE U.S.
SAFE STAFFING STANDARDS: MYTHS AND MISCONCEPTIONS
The staffing crisis in Pennsylvania hospitals is not new, and the cause is not a shortage of available RNs. In truth, our current staffing crisis is the culmination of a decades-old strategy of intentional nurse understaffing by some hospital administrators in an ultimately misguided and counterproductive effort to reduce overall costs. Short nurse staffing doesn’t reduce overall hospital costs. Likewise, safe RN staffing doesn’t increase them. That’s a myth — just one of many surrounding safe staffing standards.
MYTH: Safe nurse staffing standards would cost hospitals too much money.
FACT: Minimum staffing standards will actually save hospitals money. Sure, some hospitals would need to hire additional RNs to meet the minimum standard, but the increased costs of the additional staff would be more than offset by the money saved by the reduction in negative patient outcomes, including missed care, hospital-acquired infections, hospital readmissions, medical errors, wrong-site surgeries, failure to rescure, and death, that would result from proper staffing. In fact, a recent study on the implementation of staffing standards in Queensland, Australia, found that cost savings arising from reduced lengths of stay for patients and fewer readmissions were estimated to be more than twice the costs of additional staffing.
Plus: Negative patient outcomes due to short staffing aren’t the only monetary cost incurred by hospitals. As short-staffing leads to nurse burnout and more nurses leaving the bedside, hospitals have to hire, train, and support new RNs, which is much more costly than simply retaining nurses. In fact, the cost of replacing a single nurse can run up to $80,000.
MYTH: Government interference in the healthcare sector is never the answer. Administrators know best.
FACT: A persistent safety problem in our hospitals is absolutely the state’s concern. The 2015 report by the nonpartisan research arm of the Pennsylvania General Assembly that found that “the nurse staffing levels across Pennsylvania are highly variable and [that variability]has persisted over the last 14 years” also found that “patients exposed to even short durations of understaffing [such as from shift to shift] were at much higher risk of poor outcomes, including mortality.” That means every Pennsylvanian is at risk when unsafe staffing levels are allowed to persist in the commonwealth.
Putting in place minimum safety standards is something the government does all the time in all industries, including hospitals. Minimum staffing standards exist in nursing homes, childcare, and drug and alcohol treatment facilities. Nurse staffing in critical care is simply a blind spot.

{kind=link}
{kind=link}
{kind=link}
{kind=link}